
Evolution of Youth’s Mental Health and Quality of Life during the COVID-19 Pandemic in South Tyrol, Italy: Comparison of Two Representative Surveys

 , and
, and
Abstract
:1. Introduction
- How did mental health symptoms, especially anxiety, depression, and psychosomatic complaints, develop during the pandemic?
- Do longitudinal data only show the development of mental health symptoms, or can we derive information about changes in predictors over time?
- What are the differences between proxy-reported age groups (7–10 years and 11–19 years) in the longitudinal development of mental health problems?
- Are there groups more vulnerable to mental health problems at the local level?
2. Materials and Methods
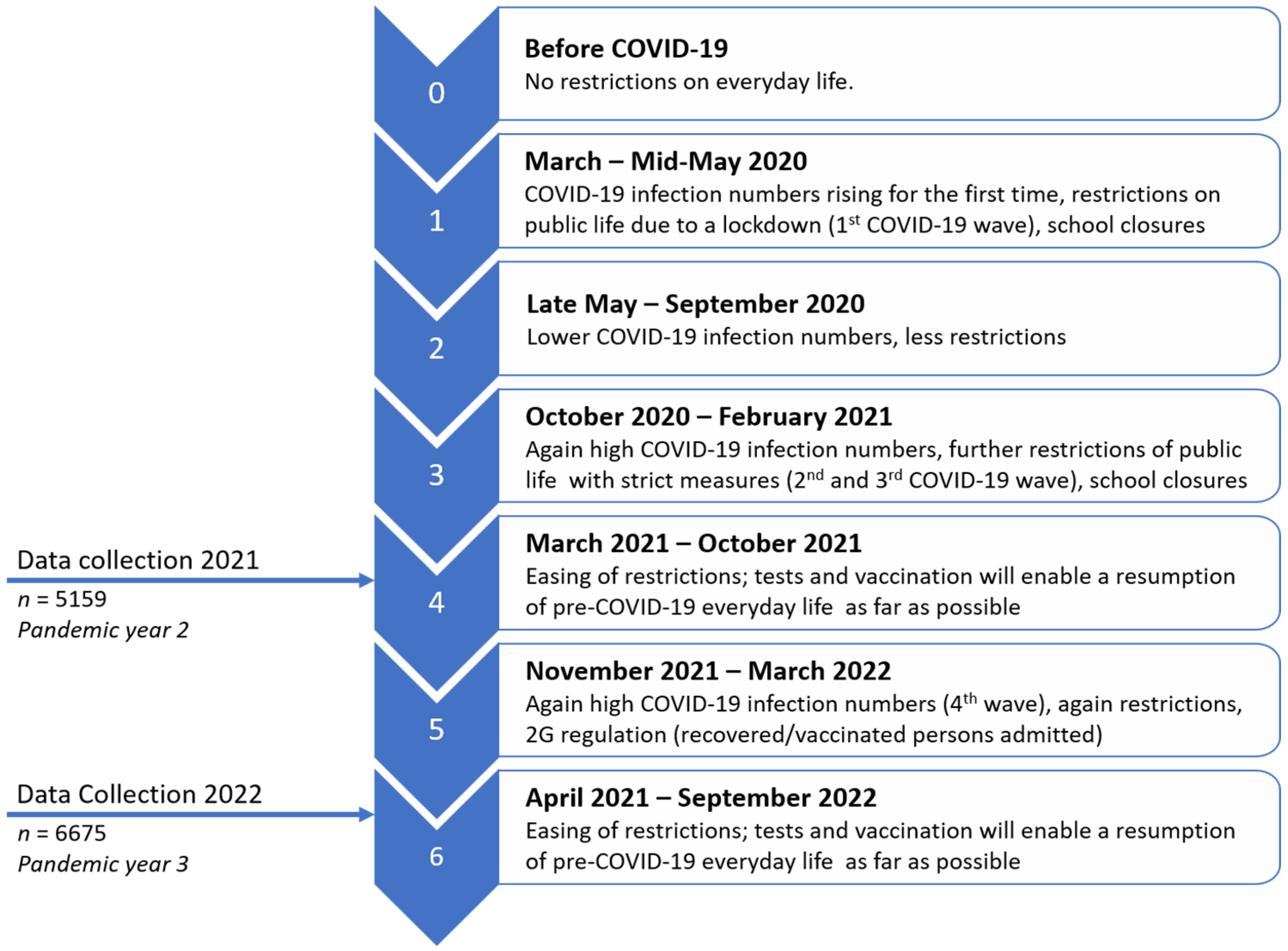
2.1. Study Design and Sample
2.2. Measures
2.2.1. Sociodemographic Variables and COVID-19 Burden
2.2.2. HRQoL and Mental Health
2.2.3. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Health-Related Quality of Life (HRQoL)
3.3. Psychosomatic Complaints (HBSC)
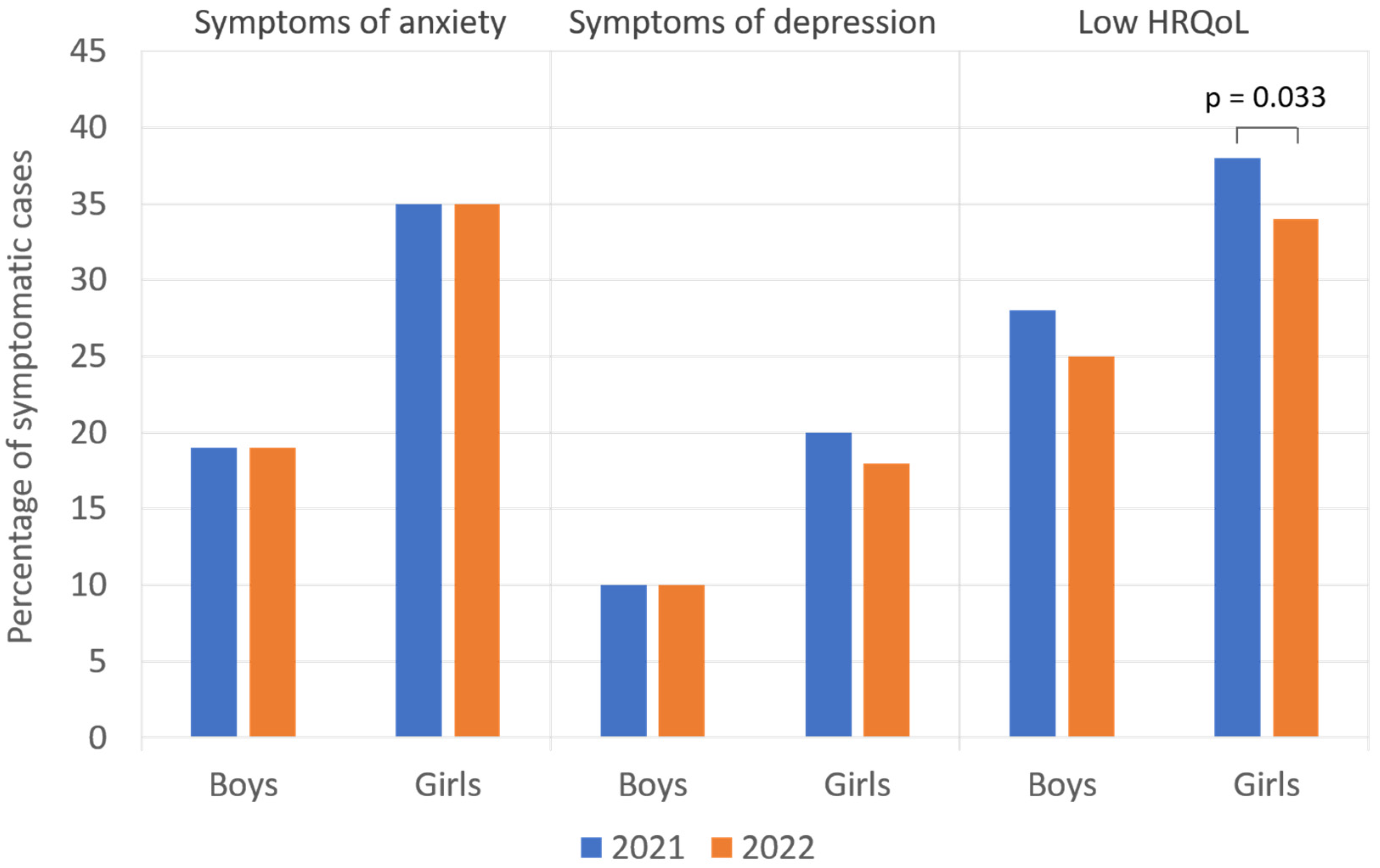
3.4. Symptoms of Anxiety and Depression
3.5. Predictors for HRQoL, Anxiety, Depressive Symptoms, and Psychosomatic Complaints
3.5.1. Correlations with Demographic Variables
- HRQoL: Self-reported HRQoL was significantly correlated with gender in 2021 (Cramer-V = 0.184, p = 0.003) and 2022 (0.165; p = 0.016), with migration background in 2021 (0.180; p = 0.02) and 2022 (0.173; p = 0.014), with single parenthood in 2021 (0.172; p = 0.026), and with living without balconies, terraces, and gardens in 2021 (0.232; p < 0.001). The proxy-reported HRQoL was significantly correlated with single parenthood in 2021 (0.111; p = 0.032) and 2022 (0.106; p = 0.017), with low parental education in 2022 (0.103; p < 0.001), and with living without balconies, terraces, and gardens in 2021 (0.151; p < 0.001).
- Anxiety: Self-reported symptoms of anxiety correlated significantly with sex in 2021 (0.251; p < 0.001) and 2022 (0.231; p < 0.001).
- Depressive symptoms: Self-reported depressive symptoms were significantly different for genders in 2021 (0.160; p < 0.001) and 2022 (0.127; p < 0.001), single parenthood in 2022 (0.088; p = 0.014), and living without balconies, terraces, and gardens in 2022 (0.087; p = 0.015).
- Psychosomatic complaints: Self-reported HBSC was significantly correlated with gender in 2021 (0.228; p < 0.001) and 2022 (0.206; p < 0.001), with low parental education in 2022 (0.164; p = 0.008), with living without balconies, terraces, or gardens in 2021 (0.182; p = 0.001), and with higher parental workload due to the pandemic in 2021 (0.200; p < 0.001) and 2022 (0.164; p = 0.015). Proxy-reported HBSC was found to differ significantly for gender in 2021 (0.113; p = 0.006) and 2022 (0.113; p = 0.001), migration background in 2021 (0.119; p = 0.004) and 2022 (0.111; p = 0.002), single parenthood in 2021 (0.107; p < 0.022) and 2022 (0.123; p < 0.001), low parental education in 2021 (0.114; p < 0.009), and living without balcony, terrace, or garden in 2021 (0.165; p < 0.001).
3.5.2. Correlations with Pandemic-Related Variables
- Parent-reported HRQoL was significantly correlated with pandemic-related predictors in 2021 and 2022: pandemic-related changes at school in 2021 (0.360; p < 0.001) and 2022 (0.350; p < 0.001); less contact with friends in 2021 (0.263; p < 0.001) and 2022 (0.284; p < 0.001); low family climate in 2021 (0.456; p < 0.001) and 2022 (0.421; p < 0.001); extended use of digital media in 2021 (0.284; p < 0.001) and 2022 (0.268; p < 0.001); children’s general burden due to the pandemic in 2021 (0.446; p < 0.001) and 2022 (0.407; p < 0.001); higher parental workload due to the pandemic in 2021 (0.191; p < 0.001) and 2022 (0.177; p < 0.001).
- Parent-reported psychosomatic complaints (HBSC) correlated significantly with pandemic-related predictors in 2021 and 2022: pandemic-related changes at school in 2021 (0.279; p < 0.001) and 2022 (0.299; p < 0.001); less contact with friends in 2021 (0.164; p < 0.001) and 2022 (0.187; p<0.001); low family climate in 2021 (0.397; p < 0.001) and 2022 (0.393; p < 0.001); extended use of digital media in 2021 (0.222; p < 0.001) and 2022 (0.219; p < 0.001); general children’s burden due to the pandemic in 2021 (0.387; p < 0.001) and 2022 (0.386; p < 0.001); higher parental workload due to the pandemic in 2021 (0.195; p < 0.001) and 2022 (0.176; p < 0.001).
- Self reported HRQoL correlated significantly with pandemic related predictors in 2021 and 2022: pandemic-related changes at school in 2021 (0.322; p < 0.001) and 2022 (0.338; p < 0.001); less contact with friends in 2021 (0.343; p < 0.001) and 2022 (0.316; p < 0.001); low family climate in 2021 (0.457; p < 0.001) and 2022 (0.409; p < 0.001); extended use of digital media in 2021 (0.235; p < 0.001) and 2022 (0.203; p < 0.001); children’s burden due to the pandemic in 2021 (0.418; p < 0.001) and 2022 (0.406; p < 0.001); higher parental workload due to the pandemic in 2021 (0.233; p < 0.001) and 2022 (0.174; p = 0.021).
- Self-reported symptoms of anxiety correlated significantly with pandemic related predictors in 2021 and 2022: pandemic-related changes at school in 2021 (0.233; p < 0.001) and 2022 (0.243; p < 0.001); less contact with friends in 2021 (0.204; p < 0.001) and 2022 (0.215; p < 0.001); low family climate in 2021 (0.274; p < 0.001) and 2022 (0.293; p < 0.001); extended use of digital media in 2021 (0.159; p < 0.001) and 2022 (0.161; p < 0.001); children’s burden due to the pandemic in 2021 (0.341; p < 0.001) and 2022 (0.346; p < 0.001); higher parental workload due to the pandemic in 2021 (0.155; p = 0.002) and 2022 (0.174; p < 0.001).
- Depressive symptoms correlated significantly with pandemic related predictors in 2021 and 2022: pandemic-related changes in 2021 (0.209; p < 0.001) and 2022 (0.238; p < 0.001); less contact with friends in 2021 (0.222; p < 0.001) and 2022 (0.245; p < 0.001); low family climate in 2021 (0.359; p < 0.001) and 2022 (0.334; p < 0.001); extended use of digital media in 2021 (0.143; p < 0.001) and 2022 (0.145; p < 0.001); general children’s burden due to the pandemic in 2021 (0.325; p < 0.001) and 2022 (0.314; p < 0.001); higher parental workload due to the pandemic in 2021 (0.12; p < 0.001) and 2022 (0.105; p = 0.002).
- Psychosomatic complaints correlated significantly with pandemic related predictors in 2021 and 2022: pandemic-related changes at school in 2021 (0.220; p < 0.001) and 2022 (0.254; p < 0.001); less contact with friends by 2021 (0.166; p = 0.013) and 2022 (0.216; p < 0.001); low family climate in 2021 (0.364; p < 0.001) and 2022 (0.366; p < 0.001); extended use of digital media in 2021 (0.219; p < 0.001) and 2022 (0.183; p < 0.001); children’s general burden due to the pandemic in 2021 (0.355; p < 0.001) and 2022 (0.345; p < 0.001); higher parental workload due to the pandemic in 2021 (0.200; p < 0.001) and 2022 (0.164; p = 0.015).
3.5.3. Linear Regression Models
3.5.4. Linear Regression Diagnostics
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents during COVID-19: A Meta-Analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Evensen, M.; Hart, R.K.; Godøy, A.A.; Hauge, L.J.; Lund, I.O.; Knudsen, A.K.S.; Grøtting, M.W.; Surén, P.; Reneflot, A. Impact of the COVID-19 Pandemic on Mental Healthcare Consultations among Children and Adolescents in Norway: A Nationwide Registry Study. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Fogarty, A.; Brown, S.; Gartland, D.; Mensah, F.; Seymour, M.; Savopoulos, P.; FitzPatrick, K.; Papadopoullos, S.; Giallo, R. Psychosocial Factors Associated with Adolescent Depressive and Anxiety Symptoms during the COVID-19 Pandemic. Int. J. Behav. Dev. 2022, 46, 308–319. [Google Scholar] [CrossRef]
- Zhu, S.; Zhuang, Y.; Lee, P.; Wong, P.W.C. The Changes of Suicidal Ideation Status among Young People in Hong Kong during COVID-19: A Longitudinal Survey. J. Affect. Disord. 2021, 294, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Brausch, A.M.; Whitfield, M.; Clapham, R.B. Comparisons of Mental Health Symptoms, Treatment Access, and Self-Harm Behaviors in Rural Adolescents before and during the COVID-19 Pandemic. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Wu, Z.; Liu, Z.; Zou, Z.; Wang, F.; Zhu, M.; Zhang, W.; Tao, H.; Ross, B.; Long, Y. Changes of Psychotic-like Experiences and Their Association with Anxiety/Depression among Young Adolescents before COVID-19 and after the Lockdown in China. Schizophr. Res. 2021, 237, 40–46. [Google Scholar] [CrossRef]
- Newlove-Delgado, T.; Russell, A.E.; Mathews, F.; Cross, L.; Bryant, E.; Gudka, R.; Ukoumunne, O.C.; Ford, T.J. Annual Research Review: The Impact of Covid-19 on Psychopathology in Children and Young People Worldwide: Systematic Review of Studies with Pre- and within-Pandemic Data. J. Child Psychol. Psychiatry 2022, 64, 611–640. [Google Scholar] [CrossRef]
- Jensen, S.S.; Reimer, D. The Effect of COVID-19-Related School Closures on Students’ Well-Being: Evidence from Danish Nationwide Panel Data. SSM-Popul. Health 2021, 16, 100945. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School Closures during Social Lockdown and Mental Health, Health Behaviors, and Well-Being among Children and Adolescents during the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Xie, X.; Liu, Q.; Zhu, K.; Jiang, Q.; Feng, Y.; Xiao, P.; Wu, X.; Song, R. Psychological Symptom Progression in School-Aged Children after COVID-19 Home Confinement: A Longitudinal Study. Front. Psychiatry 2022, 13, 809107. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Heybati, K.; Lohit, S.; Abbas, U.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; et al. Prevalence of Mental Health Symptoms in Children and Adolescents during the COVID-19 Pandemic: A Meta-Analysis. Ann. N. Y. Acad. Sci. 2023, 1520, 53–73. [Google Scholar] [CrossRef] [PubMed]
- Burdzovic Andreas, J.; Brunborg, G.S. Self-Reported Mental and Physical Health among Norwegian Adolescents Before and during the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2121934. [Google Scholar] [CrossRef] [PubMed]
- Toffolutti, V.; Plach, S.; Maksimovic, T.; Piccitto, G.; Mascherini, M.; Mencarini, L.; Aassve, A. The Association between COVID-19 Policy Responses and Mental Well-Being: Evidence from 28 European Countries. Soc. Sci. Med. 2022, 301, 114906. [Google Scholar] [CrossRef] [PubMed]
- Kurz, D.; Braig, S.; Genuneit, J.; Rothenbacher, D. Lifestyle Changes, Mental Health, and Health-Related Quality of Life in Children Aged 6–7 Years before and during the COVID-19 Pandemic in South Germany. Child Adolesc. Psychiatry Ment. Health 2022, 16, 20. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Devine, J.; Gilbert, M.; Reiss, F.; Barkmann, C.; Siegel, N.A.; Simon, A.M.; Hurrelmann, K.; Schlack, R.; et al. Child and Adolescent Mental Health During the COVID-19 Pandemic: Results of the Three-Wave Longitudinal COPSY Study. J. Adolesc. Health 2022, 71, 570–578. [Google Scholar] [CrossRef]
- Hansen, J.; Galimov, A.; Unger, J.B.; Sussman, S.Y.; Hanewinkel, R. Mental Health and Physical Complaints of German Children and Adolescents before and during the COVID-19 Pandemic: A Repeated Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 4478. [Google Scholar] [CrossRef]
- Hafstad, G.S.; Sætren, S.S.; Wentzel-Larsen, T.; Augusti, E.-M. Changes in Adolescent Mental and Somatic Health Complaints Throughout the COVID-19 Pandemic: A Three-Wave Prospective Longitudinal Study. J. Adolesc. Health 2022, 71, 406–413. [Google Scholar] [CrossRef]
- Lehmann, S.; Haug, E.; Bjørknes, R.; Mjeldheim Sandal, G.; Fadnes, L.T.; Skogen, J.C. Quality of Life among Young People in Norway during the COVID-19 Pandemic. A Longitudinal Study. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Psychological Distress Associated with the Second COVID-19 Wave: Prospective Evidence from the UK Household Longitudinal Study. J. Affect. Disord. 2022, 310, 274–278. [Google Scholar] [CrossRef]
- Moulin, F.; Bailhache, M.; Monnier, M.; Thierry, X.; Vandentorren, S.; Côté, S.M.; Falissard, B.; Simeon, T.; Geay, B.; Marchand, L.; et al. Longitudinal Impact of Psychosocial Status on Children’s Mental Health in the Context of COVID-19 Pandemic Restrictions. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Foster, S.; Estévez-Lamorte, N.; Walitza, S.; Dzemaili, S.; Mohler-Kuo, M. Perceived Stress, Coping Strategies, and Mental Health Status among Adolescents during the COVID-19 Pandemic in Switzerland: A Longitudinal Study. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef] [PubMed]
- Ertanir, B.; Kassis, W.; Garrote, A. Longitudinal Changes in Swiss Adolescent’s Mental Health Outcomes from before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 12734. [Google Scholar] [CrossRef] [PubMed]
- Bignardi, G.; Dalmaijer, E.S.; Anwyl-Irvine, A.L.; Smith, T.A.; Siugzdaite, R.; Uh, S.; Astle, D.E. Longitudinal Increases in Childhood Depression Symptoms during the COVID-19 Lockdown. Arch. Dis. Child. 2021, 106, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Bouter, D.C.; Zarchev, M.; de Neve-Enthoven, N.G.M.; Ravensbergen, S.J.; Kamperman, A.M.; Hoogendijk, W.J.G.; Grootendorst-van Mil, N.H. A Longitudinal Study of Mental Health in At-Risk Adolescents before and during the COVID-19 Pandemic. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Ehrler, M.; Hagmann, C.F.; Stoeckli, A.; Kretschmar, O.; Landolt, M.A.; Latal, B.; Wehrle, F.M. Mental Sequelae of the COVID-19 Pandemic in Children with and without Complex Medical Histories and Their Parents: Well-Being Prior to the Outbreak and at Four Time-Points throughout 2020 and 2021. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef]
- Meda, N.; Pardini, S.; Slongo, I.; Bodini, L.; Zordan, M.A.; Rigobello, P.; Visioli, F.; Novara, C. Students’ Mental Health Problems before, during, and after COVID-19 Lockdown in Italy. J. Psychiatr. Res. 2021, 134, 69–77. [Google Scholar] [CrossRef]
- Melegari, M.G.; Giallonardo, M.; Sacco, R.; Marcucci, L.; Orecchio, S.; Bruni, O. Identifying the Impact of the Confinement of COVID-19 on Emotional-Mood and Behavioural Dimensions in Children and Adolescents with Attention Deficit Hyperactivity Disorder (ADHD). Psychiatry Res. 2021, 296, 113692. [Google Scholar] [CrossRef]
- Barbieri, V.; Wiedermann, C.J.; Kaman, A.; Erhart, M.; Piccoliori, G.; Plagg, B.; Mahlknecht, A.; Ausserhofer, D.; Engl, A.; Ravens-Sieberer, U. Quality of Life and Mental Health in Children and Adolescents after the First Year of the COVID-19 Pandemic: A Large Population-Based Survey in South Tyrol, Italy. Int. J. Environ. Res. Public Health 2022, 19, 5220. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 Pandemic on Quality of Life and Mental Health in Children and Adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 31, 879–889. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Otto, C.; Devine, J.; Löffler, C.; Hurrelmann, K.; Bullinger, M.; Barkmann, C.; Siegel, N.A.; et al. Quality of Life and Mental Health in Children and Adolescents during the First Year of the COVID-19 Pandemic: Results of a Two-Wave Nationwide Population-Based Study. Eur. Child Adolesc. Psychiatry 2021, 32, 575–588. [Google Scholar] [CrossRef]
- König, W.; Lüttinger, P.; Müller, W. A Comparative Analysis of the Development and Structure of Educational Systems: Methodological Foundations and the Construction of a Comparative Educational Scale; Universität Mannheim, Institut für Sozialwissenschaften: Mannheim, Germany, 1988. [Google Scholar]
- Brauns, H.; Scherer, S.; Steinmann, S. The CASMIN Educational Classification in International Comparative Research. In Advances in Cross-National Comparison: A European Working Book for Demographic and Socio-Economic Variables; Hoffmeyer-Zlotnik, J.H.P., Wolf, C., Eds.; Springer: Boston, MA, USA, 2003; pp. 221–244. ISBN 978-1-4419-9186-7. [Google Scholar]
- Ravens-Sieberer, U.; Herdman, M.; Devine, J.; Otto, C.; Bullinger, M.; Rose, M.; Klasen, F. The European KIDSCREEN Approach to Measure Quality of Life and Well-Being in Children: Development, Current Application, and Future Advances. Qual. Life Res. 2014, 23, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.A.; Chiappetta, L.; Bridge, J.; Monga, S.; Baugher, M. Psychometric Properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A Replication Study. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Weitkamp, K.; Romer, G.; Rosenthal, S.; Wiegand-Grefe, S.; Daniels, J. German Screen for Child Anxiety Related Emotional Disorders (SCARED): Reliability, Validity, and Cross-Informant Agreement in a Clinical Sample. Child Adolesc. Psychiatry Ment. Health 2010, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, E.; Hale, W.W.; Fermani, A.; Raaijmakers, Q.; Meeus, W. Psychometric Properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in the General Italian Adolescent Population: A Validation and a Comparison between Italy and The Netherlands. J. Anxiety Disord. 2009, 23, 824–829. [Google Scholar] [CrossRef]
- Haugland, S.; Wold, B.; Stevenson, J.; Aaroe, L.E.; Woynarowska, B. Subjective Health Complaints in Adolescence. A Cross-National Comparison of Prevalence and Dimensionality. Eur. J. Public Health 2001, 11, 4–10. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- D’Argenio, P.; Minardi, V.; Mirante, N.; Mancini, C.; Cofini, V.; Carbonelli, A.; Diodati, G.; Granchelli, C.; Trinito, M.O.; Tarolla, E. Confronto tra due test per la sorveglianza dei sintomi depressivi nella popolazione. Not Ist Super Sanità 2013, 26, i–iii. [Google Scholar]
- Schuler, M.; Strohmayer, M.; Mühlig, S.; Schwaighofer, B.; Wittmann, M.; Faller, H.; Schultz, K. Assessment of Depression before and after Inpatient Rehabilitation in COPD Patients: Psychometric Properties of the German Version of the Patient Health Questionnaire (PHQ-9/PHQ-2). J. Affect. Disord. 2018, 232, 268–275. [Google Scholar] [CrossRef]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An Investigation of Mental Health Status of Children and Adolescents in China during the Outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef]
- Bussières, E.-L.; Malboeuf-Hurtubise, C.; Meilleur, A.; Mastine, T.; Hérault, E.; Chadi, N.; Montreuil, M.; Généreux, M.; Camden, C. Consequences of the COVID-19 Pandemic on Children’s Mental Health: A Meta-Analysis. Front. Psychiatry 2021, 12, 691659. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.; Xu, H.; An, N.; Zhang, P.; Liu, F.; He, S.; Hu, N.; Xiao, X.; Cui, Y.; Li, Y. The Prevalence of Mental Problems for Chinese Children and Adolescents during COVID-19 in China: A Systematic Review and Meta-Analysis. Front. Pediatr. 2021, 9, 661796. [Google Scholar] [CrossRef] [PubMed]
- Elharake, J.A.; Akbar, F.; Malik, A.A.; Gilliam, W.; Omer, S.B. Mental Health Impact of COVID-19 among Children and College Students: A Systematic Review. Child Psychiatry Hum. Dev. 2022, 54, 913–925. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Nesa, F.; Das, J.; Aggad, R.; Tasnim, S.; Bairwa, M.; Ma, P.; Ramirez, G. Global Burden of Mental Health Problems among Children and Adolescents during COVID-19 Pandemic: An Umbrella Review. Psychiatry Res. 2022, 317, 114814. [Google Scholar] [CrossRef] [PubMed]
- Listernick, Z.I.; Badawy, S.M. Mental Health Implications of the COVID-19 Pandemic Among Children and Adolescents: What Do We Know so Far? Pediatr. Health Med. Ther. 2021, 12, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Ludwig-Walz, H.; Dannheim, I.; Pfadenhauer, L.M.; Fegert, J.M.; Bujard, M. Increase of Depression among Children and Adolescents after the Onset of the COVID-19 Pandemic in Europe: A Systematic Review and Meta-Analysis. Child Adolesc. Psychiatry Ment. Health 2022, 16, 109. [Google Scholar] [CrossRef]
- Meade, J. Mental Health Effects of the COVID-19 Pandemic on Children and Adolescents: A Review of the Current Research. Pediatr. Clin. N. Am. 2021, 68, 945–959. [Google Scholar] [CrossRef]
- Ng, C.S.M.; Ng, S.S.L. Impact of the COVID-19 Pandemic on Children’s Mental Health: A Systematic Review. Front. Psychiatry 2022, 13, 975936. [Google Scholar] [CrossRef]
- De Oliveira, J.M.D.; Butini, L.; Pauletto, P.; Lehmkuhl, K.M.; Stefani, C.M.; Bolan, M.; Guerra, E.; Dick, B.; De Luca Canto, G.; Massignan, C. Mental Health Effects Prevalence in Children and Adolescents during the COVID-19 Pandemic: A Systematic Review. Worldviews Evid.-Based Nurs. 2022, 19, 130–137. [Google Scholar] [CrossRef]
- Oostrom, T.G.; Cullen, P.; Peters, S.A. The Indirect Health Impacts of the COVID-19 Pandemic on Children and Adolescents: A Review. J. Child Health Care 2022. [Google Scholar] [CrossRef]
- Saulle, R.; De Sario, M.; Bena, A.; Capra, P.; Culasso, M.; Davoli, M.; De Lorenzo, A.; Lattke, L.S.; Marra, M.; Mitrova, Z.; et al. School Closures and Mental Health, Wellbeing and Health Behaviours among Children and Adolescents during the Second COVID-19 Wave: A Systematic Review of the Literature. Epidemiol. Prev. 2022, 46, 333–352. [Google Scholar] [CrossRef] [PubMed]
- Śniadach, J.; Szymkowiak, S.; Osip, P.; Waszkiewicz, N. Increased Depression and Anxiety Disorders during the COVID-19 Pandemic in Children and Adolescents: A Literature Review. Life 2021, 11, 1188. [Google Scholar] [CrossRef] [PubMed]
- Theberath, M.; Bauer, D.; Chen, W.; Salinas, M.; Mohabbat, A.B.; Yang, J.; Chon, T.Y.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of COVID-19 Pandemic on Mental Health of Children and Adolescents: A Systematic Review of Survey Studies. SAGE Open Med. 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Chen, L.; Ran, H.; Che, Y.; Fang, D.; Sun, H.; Peng, J.; Liang, X.; Xiao, Y. Depression and Anxiety among Children and Adolescents Pre and Post COVID-19: A Comparative Meta-Analysis. Front. Psychiatry 2022, 13, 917552. [Google Scholar] [CrossRef]
- Hamatani, S.; Hiraoka, D.; Makita, K.; Tomoda, A.; Mizuno, Y. Longitudinal Impact of COVID-19 Pandemic on Mental Health of Children in the ABCD Study Cohort. Sci. Rep. 2022, 12, 19601. [Google Scholar] [CrossRef]
- Nyberg, G.; Helgadóttir, B.; Kjellenberg, K.; Ekblom, Ö. COVID-19 and Unfavorable Changes in Mental Health Unrelated to Changes in Physical Activity, Sedentary Time, and Health Behaviors among Swedish Adolescents: A Longitudinal Study. Front. Public Health 2023, 11, 1115789. [Google Scholar] [CrossRef]
- Geweniger, A.; Haddad, A.; Barth, M.; Högl, H.; Mund, A.; Insan, S.; Langer, T. Mental Health of Children with and without Special Healthcare Needs and of Their Caregivers during COVID-19: A Cross-Sectional Study. BMJ Paediatr. Open 2022, 6, e001509. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Otto, C.; Adedeji, A.; Napp, A.-K.; Becker, M.; Blanck-Stellmacher, U.; Löffler, C.; Schlack, R.; Hölling, H.; et al. Mental health and psychological burden of children and adolescents during the first wave of the COVID-19 pandemic-results of the COPSY study. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 1512–1521. [Google Scholar] [CrossRef]
- Schlack, R.; Neuperdt, L.; Hölling, H.; De Bock, F.; Ravens-Sieberer, U.; Mauz, E.; Wachtler, B.; Beyer, A.-K. Impact of the COVID-19 Pandemic and the Related Containment Measures on the Mental Health of Children and Adolescents. J. Health Monit. 2020, 5, 21–31. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Devine, J.; Napp, A.-K.; Kaman, A.; Saftig, L.; Gilbert, M.; Reiss, F.; Löffler, C.; Simon, A.; Hurrelmann, K.; et al. Three Years into the Pandemic: Results of the Longitudinal German COPSY Study on Youth Mental Health and Health-Related Quality of Life. SSRN. 2023. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4304666 (accessed on 10 March 2023).
- Platt, B.; Danzer, V.; Schulte-Körne, G. Critical Reflections on the Manuscript “Impact of the COVID-19 Pandemic on Quality of Life and Mental Health in Children and Adolescents in Germany” Published in ECAP on January 25th 2021. Eur. Child Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef]
- Wenter, A.; Schickl, M.; Sevecke, K.; Juen, B.; Exenberger, S. Children’s Mental Health During the First Two Years of the COVID-19 Pandemic: Burden, Risk Factors and Posttraumatic Growth-A Mixed-Methods Parents’ Perspective. Front. Psychol 2022, 13, 901205. [Google Scholar] [CrossRef] [PubMed]
- Sevecke, K.; Wenter, A.; Haid-Stecher, N.; Fuchs, M.; Böge, I. A three-country comparison of mental health and treatment options of children and adolescents with mental health problems in times after the COVID-19 pandemic. Neuropsychiatrie 2022, 36, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.J.; Barblan, L.P.; Lory, I.; Landolt, M.A. Age-Related Effects of the COVID-19 Pandemic on Mental Health of Children and Adolescents. Eur. J. Psychotraumatol. 2021, 12, 1901407. [Google Scholar] [CrossRef]
- Babore, A.; Trumello, C.; Lombardi, L.; Candelori, C.; Chirumbolo, A.; Cattelino, E.; Baiocco, R.; Bramanti, S.M.; Viceconti, M.L.; Pignataro, S.; et al. Mothers’ and Children’s Mental Health During the COVID-19 Pandemic Lockdown: The Mediating Role of Parenting Stress. Child Psychiatry Hum. Dev. 2021, 54, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Vicari, S.; Pontillo, M. Developmental Psychopathology in the COVID-19 Period. COVID-19 Pandemic Impact on Children and Adolescents’ Mental Health. Psychiatr. Danub. 2021, 33, 33–35. [Google Scholar]
- Weierstall-Pust, R.; Schnell, T.; Heßmann, P.; Feld, M.; Höfer, M.; Plate, A.; Müller, M.J. Stressors Related to the COVID-19 Pandemic, Climate Change, and the Ukraine Crisis, and Their Impact on Stress Symptoms in Germany: Analysis of Cross-Sectional Survey Data. BMC Public Health 2022, 22, 2233. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| COP-S 2021 | COP-S 2022 | p-Value | |||
|---|---|---|---|---|---|
| (n = 5169) | (n = 6665) | ||||
| n (%) | M (SD) | n (%) | M (SD) | ||
| Age | 12.0 (3.58) | 12.21 (3.58) | <0.001 | ||
| 7–10 years | 2025 (39.2) | 2432 (36.5) | 0.003 | ||
| 11–19 years | 3144 (60.8) | 4233 (63.5) | |||
| Gender | |||||
| Male | 2560 (49.5) | 3277 (49.2) | n.s. | ||
| Female | 2609 (50.5) | 3388 (50.8) | |||
| Age of the parent, years | 44.4 (6.4) | 44.7 (6.2) | 0.002 | ||
| Gender of the parents, male | 597 (11.5) | 748 (11.2) | n.s. | ||
| Migration background | |||||
| No | 4045 (88.4) | 5200 (88.7) | n.s. | ||
| Yes | 533 (11.6) | 660 (11.3) | |||
| Parental education | |||||
| Low | 1134 (23.0) | 1315 (20.6) | 0.002 | ||
| Moderate/high | 3802 (77.0) | 5078 (79.4) | |||
| Single parenthood | |||||
| No | 4603 (91.7) | 6033 (91.2) | n.s. | ||
| Yes | 419 (8.3) | 579 (8.8) | |||
| Live without balcony, terrasse, garden | |||||
| Yes | 82 (1.6) | 140 (2.2) | |||
| No | 4950 (98.4) | 6318 (97.8) | 0.038 | ||
| Survey | Self-Reported | Parent-Reported | |||||
|---|---|---|---|---|---|---|---|
| n | Low HRQoL 1 | Normal/High HRQoL 1 | n | Low HRQoL 1 | Normal/High HRQoL 1 | ||
| Boys | COP-S 2021 | 920 | 254 (27.6) | 666 (72.4) | 1280 | 391 (30.5) | 889 (69.5) |
| COP-S 2022 | 1004 | 251 (25) | 753 (75) | 1605 | 401 (25) | 1204 (75) | |
| p-value 2 | n.s. | 0.001 | |||||
| Girls | COP-S 2021 | 983 | 374 (38) | 609 (62) | 1324 | 443 (33.5) | 881 (66.5) |
| COP-S 2022 | 1076 | 361 (33.6) | 715 (66.4) | 1665 | 433 (26) | 1232 (74) | |
| p-value 2 | 0.033 | <0.001 | |||||
| Boys and girls | COP-S 2021 | 1903 | 628 (33) | 1275 (67) | 2604 | 834 (32) | 1770 (68) |
| COP-S 2022 | 2080 | 612 (29.4) | 1468 (70.6) | 3270 | 834 (25.5) | 2436 (74.5) | |
| p-value 2 | 0.015 | <0.001 | |||||
| Age (Years) | Self (%) | Proxy (%) | |||
|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | ||
| Headache | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 19.6 | 22.9 |
| 11–19 | 32.0 | 47.8 | 28.2 | 39.4 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 22.6 | 28.0 |
| 11–19 | 36.3 | 51.1 | 31.9 | 45.8 | |
| p-values 1 | n.d./*** | **/*** | |||
| p-values 2 | n.d./* | n.d./n.s. | n.s./* | */*** | |
| Abdominal pain | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 25.6 | 29.6 |
| 11–19 | 23.5 | 40.3 | 21.4 | 33.9 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 28.0 | 34.2 |
| 11–19 | 26.7 | 41.7 | 22.7 | 36.3 | |
| p-values 1 | n.d./*** | **/*** | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | n.s./n.s. | */n.s. | |
| Backache | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 4.6 | 6.3 |
| 11–19 | 25.9 | 32.4 | 17.7 | 21.6 | |
| p-values 1 | n.d./** | n.s./* | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 6.8 | 6.6 |
| 11–19 | 25.5 | 33.1 | 18.3 | 23.4 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | */n.s. | n.s./n.s. | |
| Feeling low | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 28.8 | 26.3 |
| 11–19 | 34.6 | 48.5 | 32.2 | 42.4 | |
| p-values 1 | n.d/*** | n.s/*** | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 25.4 | 24.7 |
| 11–19 | 35.0 | 50.8 | 35.1 | 44.9 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | n.s./n.s. | n.s./n.s. | |
| Dizziness | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 5.4 | 5.5 |
| 11–19 | 15.9 | 25.9 | 9.8 | 15.9 | |
| p-values 1 | n.d/*** | n.s/*** | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 5.5 | 5.9 |
| 11–19 | 16.8 | 25.0 | 11.0 | 15.9 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | n.s./n.s. | n.s./n.s. | |
| Irritable | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 62.0 | 60.4 |
| 11–19 | 55.7 | 66.8 | 64.5 | 69.5 | |
| p-values 1 | n.d./*** | n.s./** | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 57.0 | 56.1 |
| 11–19 | 52.4 | 63.9 | 59.1 | 65.9 | |
| p-values 1 | n.d./*** | n.s./*** | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | */** | n.s./* | |
| Feeling nervous | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 37.1 | 30.8 |
| 11–19 | 39.6 | 49.6 | 42.0 | 42.8 | |
| p-values 1 | n.d/*** | **/n.s | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 35.0 | 28.5 |
| 11–19 | 43.4 | 47.9 | 40.8 | 42.6 | |
| p-values 1 | n.d./* | **/n.s. | |||
| p-values 2 | n.d/n.s. | n.d./n.s. | n.s./n.s. | n.s./n.s. | |
| Sleeping difficulties | |||||
| COP-S 2021 | 7–10 | n.d. | n.d. | 34.1 | 38.8 |
| 11–19 | 38.8 | 45.0 | 31.2 | 37.7 | |
| p-values 1 | n.d./** | n.s./* | |||
| COP-S 2022 | 7–10 | n.d. | n.d. | 26.9 | 32.7 |
| 11–19 | 36.8 | 43.7 | 31.7 | 35.2 | |
| p-values 1 | n.d./** | **/* | |||
| p-values 2 | n.d./n.s. | n.d./n.s. | **/n.s. | **/n.s. | |
| HRQoL 1 | Anxiety 3,4 | Depressive Symptoms 3,4 | Psychosomatic Complaints | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proxy-Report 2 | Self-Report 4 | COP-S 2021 | COP-S 2022 | COP-S 2021 | COP-S 2022 | Proxy-Report 2,5 | Self-Report 4,5 | |||||
| COP-S 2021 | COP-S 2022 | COP-S 2021 | COP-S 2022 | COP-S 2021 | COP-S 2022 | COP-S 2021 | COP-S 2022 | |||||
| Intercept | 62.080 *** | 60.944 *** | 58.910 *** | 54.914 *** | 2.5192 *** | 3.255 *** | −0.917 *** | −0.757 *** | 41.000 *** | 38.486 *** | 41.643 *** | 39.484 *** |
| Age | −0.334 *** | −0.370 *** | 0.092 *** | 0.090 *** | −0.178 *** | −0.264 *** | −0.127 * | |||||
| Female | ||||||||||||
| Female × age | −0.175 *** | −0.120 *** | 0.148 *** | 0.117 *** | 0.027 *** | 0.018 *** | −0.068 *** | −0.061 *** | −0.145 *** | −0.117 ** | ||
| Migration background | −1.716 * | −0.780 * | ||||||||||
| Single parenthood | −1.826 * | −1.142 * | −1.114 * | −1.372 ** | ||||||||
| Low parental education | 0.661 * | |||||||||||
| Living without balcony, terrace, garden | ||||||||||||
| Parents’ burden due to pandemic | −1.597 *** | −1.068 ** | −1.680 ** | 0.728 ** | 0.630 ** | 0.150 * | −1.084 *** | −0.613 ** | −0.801 ** | |||
| Children’s burden due to situation at school | −4.439 *** | −4.281 *** | −3.730 *** | −4.472 *** | 1.056 *** | 1.210 *** | 0.267 *** | 0.360 *** | −1.030 *** | −1.372 ** | −0.932 ** | −1.527 *** |
| Less contact with friends | −3.234 *** | −3.060 *** | −4.376 *** | −3.833 *** | 0.988 ** | 0.962 ** | 0.273 ** | 0.383 *** | −0.893 * | −0.510 * | ||
| Lower family climate | −7.680 *** | −6.899 *** | −7.369 *** | −6.874 *** | 2.240 *** | 2.611 *** | 0.992 *** | 0.929 *** | −3.076 *** | −2.508 *** | −3.556 *** | −3.722 *** |
| Extended use of digital media | −2.919 *** | −2.672 *** | −1.716 ** | |||||||||
| Model fit (Adjusted R2) | 0.285 | 0.255 | 0.275 | 0.224 | 0.161 | 0.162 | 0.202 | 0.178 | 0.183 | 0.156 | 0.163 | 0.167 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbieri, V.; Wiedermann, C.J.; Piccoliori, G.; Mahlknecht, A.; Plagg, B.; Ausserhofer, D.; Ravens-Sieberer, U.; Engl, A. Evolution of Youth’s Mental Health and Quality of Life during the COVID-19 Pandemic in South Tyrol, Italy: Comparison of Two Representative Surveys. Children 2023, 10, 895. https://doi.org/10.3390/children10050895
Barbieri V, Wiedermann CJ, Piccoliori G, Mahlknecht A, Plagg B, Ausserhofer D, Ravens-Sieberer U, Engl A. Evolution of Youth’s Mental Health and Quality of Life during the COVID-19 Pandemic in South Tyrol, Italy: Comparison of Two Representative Surveys. Children. 2023; 10(5):895. https://doi.org/10.3390/children10050895
Chicago/Turabian StyleBarbieri, Verena, Christian J. Wiedermann, Giuliano Piccoliori, Angelika Mahlknecht, Barbara Plagg, Dietmar Ausserhofer, Ulrike Ravens-Sieberer, and Adolf Engl. 2023. "Evolution of Youth’s Mental Health and Quality of Life during the COVID-19 Pandemic in South Tyrol, Italy: Comparison of Two Representative Surveys" Children 10, no. 5: 895. https://doi.org/10.3390/children10050895