
Effects of an Interdisciplinary Approach in the Management of Temporomandibular Disorders: A Scoping Review

 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Review Inclusion Criteria
2.3. Selection Criteria and Data Extraction
2.4. Methodological Quality and Risk of Bias Assessment
3. Results
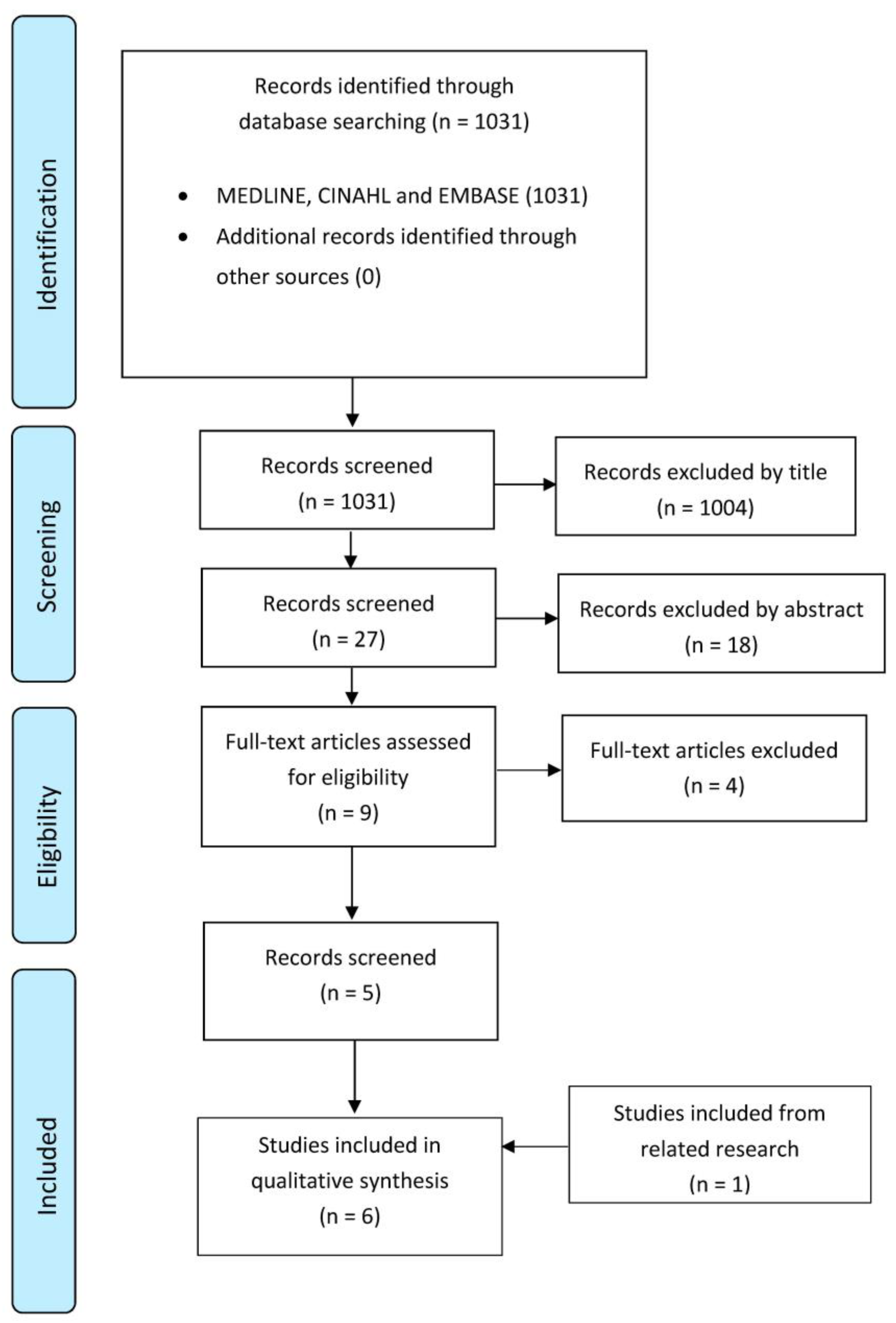
3.1. Study Selection
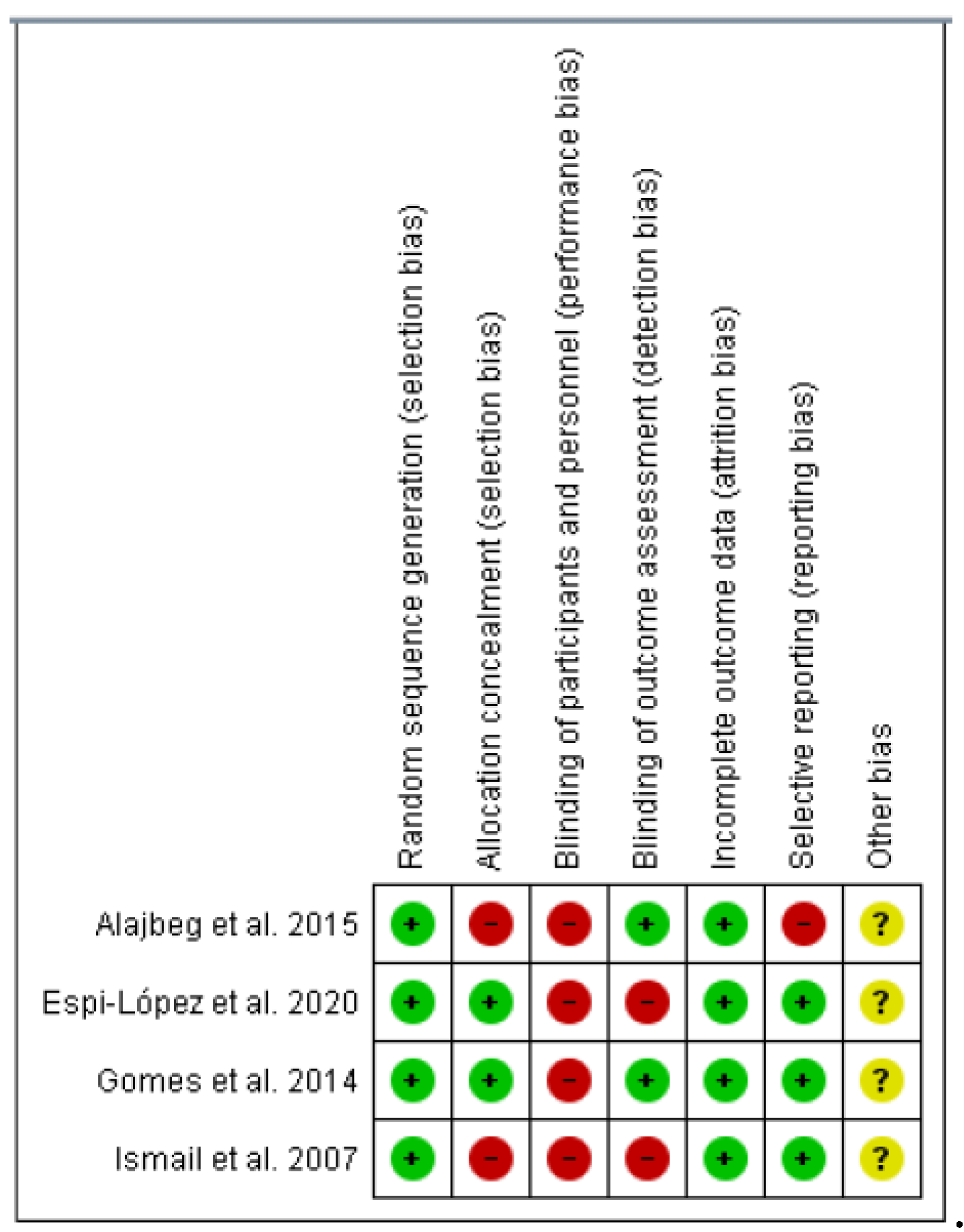
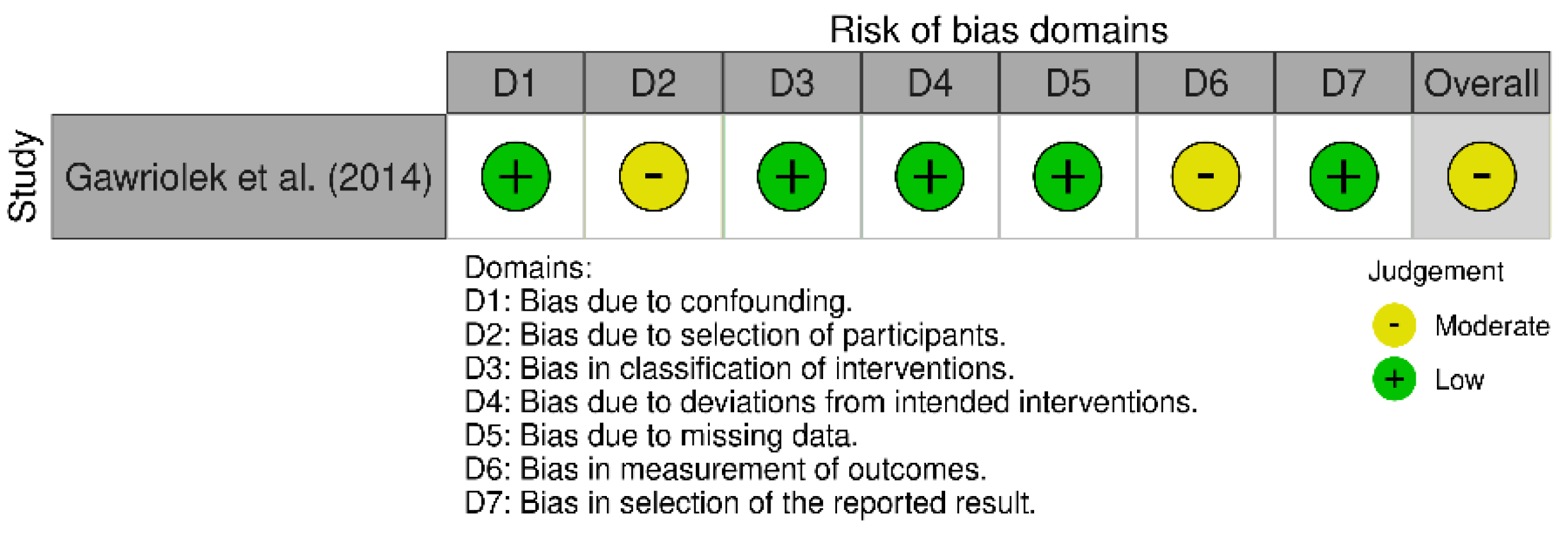
3.2. Risk of Bias within and across the Studies
3.3. Quality Assessment
3.4. Studies Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tanaka, E.; Detamore, M.S.; Mercuri, L.G. Degenerative disorders of the temporomandibular joint: Etiology, diagnosis, and treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R. Executive summary of the Diagnostic Criteria for Temporomandibular Disorders for clinical and research applications. J. Am. Dent. Assoc. 2016, 147, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Romero, E.A.; Melendez Oliva, E.; Alonso Perez, J.L.; Martin Perez, S.; Turroni, S.; Marchese, L.; Villafane, J.H. Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature. Nutrients 2021, 13, 716. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis-Review of the Literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef]
- Diaz-Saez, M.; Saenz-Jimenez, C.; Villafane, J.H.; Paris-Alemany, A.; La Touche, R. Hypoalgesic and Motor Effects of Neural Mobilisation versus Soft-Tissue Interventions in Experimental Craniofacial Hyperalgesia: A Single-Blinded Randomised Controlled Trial. J. Clin. Med. 2021, 10, 4434. [Google Scholar] [CrossRef]
- Kalladka, M.; Young, A.; Khan, J. Myofascial pain in temporomandibular disorders: Updates on etiopathogenesis and management. J. Bodyw. Mov. Ther. 2021, 28, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Kietrys, D.M.; Palombaro, K.M.; Mannheimer, J.S. Dry needling for management of pain in the upper quarter and craniofacial region. Curr. Pain Headache Rep. 2014, 18, 437. [Google Scholar] [CrossRef]
- Miernik, M.; Wieckiewicz, W. The Basic Conservative Treatment of Temporomandibular Joint Anterior Disc Displacement Without Reduction--Review. Adv. Clin. Exp. Med. Off. Organ Wroc. Med. Univ. 2015, 24, 731–735. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Boening, K.; Wiland, P.; Shiau, Y.Y. Paradowska-Stolarz A: Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J. Headache Pain 2015, 16, 106. [Google Scholar] [CrossRef]
- La Touche, R.; Perez-Fernandez, M.; Barrera-Marchessi, I.; Lopez-de-Uralde-Villanueva, I.; Villafane, J.H.; Prieto-Aldana, M.; Suso-Marti, L. Paris-Alemany A: Psychological and physical factors related to disability in chronic low back pain. J. Back Musculoskelet. Rehabil. 2019, 32, 603–611. [Google Scholar] [CrossRef]
- Ortego, G.; Villafane, J.H.; Domenech-Garcia, V.; Berjano, P.; Bertozzi, L.; Herrero, P. Is there a relationship between psychological stress or anxiety and chronic nonspecific neck-arm pain in adults? A systematic review and meta-analysis. J. Psychosom. Res. 2016, 90, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Langella, F.; Fusini, F.; Rossi, G.; Villafane, J.H.; Migliaccio, N.; Donzelli, S.; Berjano, P. Spinal deformity and malocclusion association is not supported by high-quality studies: Results from a systematic review of the literature. Eur. Spine J. 2019, 28, 1638–1651. [Google Scholar] [CrossRef] [PubMed]
- De Lima, E.S.R.F.; Vanti, C.; Banchelli, F.; Trani Brandao, J.G.; Oliveira Amorim, J.B.; Villafane, J.H.; Guccione, A.; Pillastrini, P. The effect of Global Postural Reeducation on body weight distribution in sitting posture and on musculoskeletal pain. A pilot study. Med. Lav. 2017, 108, 187–196. [Google Scholar]
- Parazza, S.; Vanti, C.; O’Reilly, C.; Villafane, J.H. Tricas Moreno JM, Estebanez De Miguel E: The relationship between cervical flexor endurance, cervical extensor endurance, VAS, and disability in subjects with neck pain. Chiropr. Man. Ther. 2014, 22, 10. [Google Scholar] [CrossRef]
- Sherrington, C.; Herbert, R.D.; Maher, C.G.; Moseley, A.M. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man. Ther. 2000, 5, 223–226. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Alajbeg, I.Z.; Gikic, M.; Valentic-Peruzovic, M. Mandibular Range of Movement and Pain Intensity in Patients with Anterior Disc Displacement without Reduction. Acta Stomatol. Croat. 2015, 49, 119–127. [Google Scholar] [CrossRef] [PubMed]
- de Toledo, E.G., Jr.; Silva, D.P.; de Toledo, J.A.; Salgado, I.O. The interrelationship between dentistry and physiotherapy in the treatment of temporomandibular disorders. J. Contemp. Dent. Pract. 2012, 13, 579–583. [Google Scholar] [CrossRef]
- Espi-Lopez, G.V.; Arnal-Gomez, A.; Cuerda Del Pino, A.; Benavent-Corai, J.; Serra-Ano, P.; Ingles, M. Effect of Manual Therapy and Splint Therapy in People with Temporomandibular Disorders: A Preliminary Study. J. Clin. Med. 2020, 9, 2411. [Google Scholar] [CrossRef]
- Gawriolek, K.; Azer, S.S.; Gawriolek, M.; Piotrowski, P.R. Mandibular function after Myorelaxation Therapy in temporomandibular disorders. Adv. Med. Sci. 2015, 60, 6–12. [Google Scholar] [CrossRef]
- Gomes, C.A.; El Hage, Y.; Amaral, A.P.; Politti, F.; Biasotto-Gonzalez, D.A. Effects of massage therapy and occlusal splint therapy on electromyographic activity and the intensity of signs and symptoms in individuals with temporomandibular disorder and sleep bruxism: A randomized clinical trial. Chiropr. Man. Ther. 2014, 22, 43. [Google Scholar] [CrossRef] [Green Version]
- Ismail, F.; Demling, A.; Hessling, K.; Fink, M.; Stiesch-Scholz, M. Short-term efficacy of physical therapy compared to splint therapy in treatment of arthrogenous TMD. J. Oral Rehabil. 2007, 34, 807–813. [Google Scholar] [CrossRef]
- Herrera-Valencia, A.; Ruiz-Munoz, M.; Martin-Martin, J.; Cuesta-Vargas, A.; Gonzalez-Sanchez, M. Effcacy of Manual Therapy in TemporomandibularJoint Disorders and Its Medium-and Long-TermEffects on Pain and Maximum Mouth Opening: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3404. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, L.; Wu, D.; Yu, C.; Fan, S.; Cai, B. Effectiveness of exercise therapy versus occlusal splint therapy for the treatment of painful temporomandibular disorders: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 6122–6132. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, P.; Trybulec, B.; Pihut, M. The Application of Manual Techniques in Masticatory Muscles Relaxation as Adjunctive Therapy in the Treatment of Temporomandibular Joint Disorders. Int. J. Environ. Res. Public Health 2021, 18, 12970. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Wolford, L.M.; Ellis, E., 3rd; Neff, A. The hierarchy of different treatments for arthrogenous temporomandibular disorders: A network meta-analysis of randomized clinical trials. J. Cranio-Maxillo-Facial Surg. 2020, 48, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Kietrys, D.M.; Palombaro, K.M.; Azzaretto, E.; Hubler, R.; Schaller, B.; Schlussel, J.M.; Tucker, M. Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J. Orthop. Sport. Phys. Ther. 2013, 43, 620–634. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Goulet, J.P.; El-Ouazzani, M.; Turgeon, A.F. Temporomandibular Lavage Versus Nonsurgical Treatments for Temporomandibular Disorders: A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 1352–1362. [Google Scholar] [CrossRef]
- Vos, L.M.; Huddleston Slater, J.J.; Stegenga, B. Lavage therapy versus nonsurgical therapy for the treatment of arthralgia of the temporomandibular joint: A systematic review of randomized controlled trials. J. Orofac. Pain 2013, 27, 171–179. [Google Scholar] [CrossRef]
- Agius, A.M.; Jones, N.S.; Muscat, R. A Randomized Controlled Trial comparing the efficacy of low-dose amitriptyline, amitriptyline with pindolol and surrogate placebo in the treatment of chronic tension-type facial pain. Rhinology 2013, 51, 143–153. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Pitance, L.; Singh, V.; Neto, F.; Thie, N.; Michelotti, A. Effectiveness of Manual Therapy and Therapeutic Exercise for Temporomandibular Disorders: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 9–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitroulis, G.; Gremillion, H.A.; Dolwick, M.F.; Walter, J.H. Temporomandibular disorders. 2. Non-surgical treatment. Aust. Dent. J. 1995, 40, 372–376. [Google Scholar] [CrossRef]
- Diracoglu, D.; Saral, I.B.; Keklik, B.; Kurt, H.; Emekli, U.; Ozcakar, L.; Karan, A.; Aksoy, C. Arthrocentesis versus nonsurgical methods in the treatment of temporomandibular disc displacement without reduction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Firmani, M.; Miralles, R.; Casassus, R. Effect of lidocaine patches on upper trapezius EMG activity and pain intensity in patients with myofascial trigger points: A randomized clinical study. Acta Odontol. Scand. 2015, 73, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Gewandter, J.S.; McDermott, M.P.; McKeown, A.; Hoang, K.; Iwan, K.; Kralovic, S.; Rothstein, D.; Gilron, I.; Katz, N.P.; Raja, S.N.; et al. Reporting of cross-over clinical trials of analgesic treatments for chronic pain: Analgesic, Anesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks systematic review and recommendations. Pain 2016, 157, 2544–2551. [Google Scholar] [CrossRef]
- Haggman-Henrikson, B.; Alstergren, P.; Davidson, T.; Hogestatt, E.D.; Ostlund, P.; Tranaeus, S.; Vitols, S.; List, T. Pharmacological treatment of oro-facial pain—Health technology assessment including a systematic review with network meta-analysis. J. Oral Rehabil. 2017, 44, 800–826. [Google Scholar] [CrossRef]
- List, T.; Axelsson, S. Management of TMD: Evidence from systematic reviews and meta-analyses. J. Oral Rehabil. 2010, 37, 430–451. [Google Scholar] [CrossRef]
- McNeely, M.L.; Armijo Olivo, S.; Magee, D.J. A systematic review of the effectiveness of physical therapy interventions for temporomandibular disorders. Phys. Ther. 2006, 86, 710–725. [Google Scholar] [CrossRef]
- Medlicott, M.S.; Harris, S.R. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder. Phys. Ther. 2006, 86, 955–973. [Google Scholar] [CrossRef]
- Mujakperuo, H.R.; Watson, M.; Morrison, R.; Macfarlane, T.V. Pharmacological interventions for pain in patients with temporomandibular disorders. Cochrane Database Syst. Rev. 2010, 10, CD004715. [Google Scholar] [CrossRef]
- Scrivani, S.J.; Keith, D.A.; Kaban, L.B. Temporomandibular disorders. N. Engl. J. Med. 2008, 359, 2693–2705. [Google Scholar] [CrossRef]
- Stegenga, B.; de Bont, L.G.; Dijkstra, P.U.; Boering, G. Short-term outcome of arthroscopic surgery of temporomandibular joint osteoarthrosis and internal derangement: A randomized controlled clinical trial. Br. J. Oral Maxillofac. Surg. 1993, 31, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Syrop, S.B. Initial management of temporomandibular disorders. Dent. Today 2002, 21, 52–57. [Google Scholar] [PubMed]
- White, A.P.; Arnold, P.M.; Norvell, D.C.; Ecker, E.; Fehlings, M.G. Pharmacologic management of chronic low back pain: Synthesis of the evidence. Spine 2011, 36 (Suppl. S21), S131–S143. [Google Scholar] [CrossRef] [PubMed]
- Malgorzata, P.; Malgorzata, K.M.; Karolina, C.; Gala, A. Diagnostic of Temporomandibular Disorders and Other Facial Pain Conditions-Narrative Review and Personal Experience. Medicina 2020, 56, 472. [Google Scholar] [CrossRef] [PubMed]
- Visscher, C.M.; Lobbezoo, F.; de Boer, W.; van der Zaag, J.; Naeije, M. Prevalence of cervical spinal pain in craniomandibular pain patients. Eur. J. Oral Sci. 2001, 109, 76–80. [Google Scholar] [CrossRef]
- Anokhina, A.V.; Yakhin, K.K.; Sayfullina, A.R.; Silantyeva, E.N.; Abzalova, S.L. On the role of psychological disorders in the development of the syndrome of pain dysfunction of the temporomandibular joint. Stomatologiia 2021, 100, 115–119. [Google Scholar] [CrossRef]
- Osses-Anguita, Á.E.; Sánchez-Sánchez, T.; Soto-Goñi, X.A.; García-González, M.; Alén Fariñas, F.; Cid-Verdejo, R.; Sánchez Romero, E.A.; Jiménez-Ortega, L. Awake and Sleep Bruxism Prevalence and Their Associated Psychological Factors in First-Year University Students: A Pre-Mid-Post COVID-19 Pandemic Comparison. Int. J. Environ. Res. Public Health 2023, 20, 2452. [Google Scholar] [CrossRef]
- Sánchez Romero, E.A.; Martínez-Pozas, O.; García-González, M.; de-Pedro, M.; González-Álvarez, M.E.; Esteban-González, P.; Cid-Verdejo, R.; Villafañe, J.H. Association between Sleep Disorders and Sleep Quality in Patients with Temporomandibular Joint Osteoarthritis: A Systematic Review. Biomedicines 2022, 10, 2143. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors, Years | Aim of the Study | Study Design, Participants, Methods | Outcomes + Follow-Up | Results | Conclusions | Quality Score |
|---|---|---|---|---|---|---|
| Ismail et al. [22] (2007) | To evaluate the efficacy of physical therapy, in addition to splint therapy, on treatment outcomes in patients with TMD with respect to objective and subjective parameters. | Study design: RCT N: 26 patients diagnosed with TMD.
| Jaw mobility Active and passive maximum jaw opening Pain Visual Analogue Scale (VAS)
Follow-up: 1, 4, 8, and 12 weeks | Compared with the baseline, in both groups, mandibular movement capacity increased significantly after treatment, whereas subjective pain decreased significantly (p < 0.05). After therapy, the difference in active jaw opening between groups was significant (p < 0.05). | Physiotherapy, combined with occlusal splint therapy, appears to positively affect the treatment outcome of patients with TMD. | PEDro 5/10 |
| Gomes et al. [21] (2014) | To evaluate the effects of manual therapy and occlusal splints on the electromyographic activity and signs and symptoms of patients with severe TMD. | Study design: RCT N: 60 participants diagnosed with TMD were randomly distributed into 4 groups. (1) massage group. (2) conventional occlusal splint group. (3) massage group + conventional occlusal splint group. (4) silicone occlusal splint group. | Electromyographic activity Surface EMG (right and left masseter and anterior temporal muscles) Follow-up: None, only pre- and post-treatment evaluations | All groups had a statistically significant improvement compared to before the intervention. Comparing the groups, only the group that combined manual therapy with occlusal splinting had a statistically significant improvement (p < 0.05). | The combination of massage and conventional occlusal splinting reduced the intensity of signs and symptoms among individuals with severe TMD. | PEDro 7/10 |
| Alajbeg et al. [17] (2015) | The hypothesis tested was that the simultaneous use of an occlusal splint and physical therapy is an effective treatment of anterior disc displacement without reduction (TMD). | Study design: RCT N: 12 participants with anterior disc displacement without reduction (TMD) were randomly assigned into 2 groups:
| Pain Visual Analogue Scale (VAS) for spontaneous pain Pain-free opening and path of mouth opening Maximum comfortable opening (MCO) Maximum assisted opening (MAO) Opening pattern Follow-up: 1 month, 3 months, and 6 months | Regarding VAS scores, group II had a greater improvement (p = 0.0001) than group I (p = 0.001). Jaw opening with and without pain improved significantly only in group II (maximum opening without pain p = 0.006, maximum opening with pain p = 0.004). The use of the occlusal splint alone did not lead to statistically significant changes in the range of mouth opening (p > 0.05). | The simultaneous use of an occlusal splint and physiotherapy improved the range of mouth opening more effectively than the occlusal splint used alone. Both treatment options were effective in reducing pain. | PEDro 6/10 |
| Espí-López et al. [19] (2020) | To ascertain whether a combined program of manual therapy techniques, including intraoral treatment, plus traditional splint therapy improves pain and clinical dysfunction in subjects with TMD. | Study design: RCT N: 16 participants with TMD were assigned to either the manual therapy plus splint—experimental group (EG, n = 8) or the splint therapy alone—control group (CG, n = 8). | Pain Visual Analogue Scale (VAS) Pain pressure threshold (PPT) Minimal pressure which induces pain (pressure algometry) Dysfunction Index of TMD Helkimo Index Change perception Patient Global Impression of Change Scale (PGICS) Follow-up: 1 month | EG showed a significant reduction in pain, higher pain pressure threshold, significant improvement of dysfunction, and significantly positive perception of change after treatment (p < 0.05 all). The between-group differences were statistically significant. | Manual therapy plus splint therapy showed a reduction in perceived pain (3-point decrease), higher pain pressure threshold (of at least 1.0 kg/cm2), and improvement of disability caused by pain (4.4-point decrease), compared to splint therapy alone. | PEDro 6/10 |
| Toledo Jr et al. [18] (2012) | This study aims to evaluate the effectiveness of interdisciplinary work between dentistry and physiotherapy in determining the treatment plan for patients with TMD. | Study design: A retrospective cohort study N: 300 patient records from the ATM service file. Three factors were analyzed: (1) The physiotherapy techniques used. (2) Guidelines or procedures for home exercises. (3) the temporomandibular joint (TMJ) palpation pain rates (VAS). | Temporomandibular joint pain rates Visual Analogue Scale (VAS) | The initial analysis of pain on palpation showed that 151 patients (50.3%) had a high level of pain (grade III), 92 (30.7%) had a moderate level of pain (grade II), 39 (13%) had a low level of pain (grade I), and 18 (6%) had no pain. Considering the final pain on palpation, 13 patients (4.3%) had grade III, 22 (7.3%) grade II, 63 (21%) grade I, and 202 (67.3%) were without pain. | It is essential to have an interdisciplinary treatment plan, where physical therapy helps pain relief and dentistry treat the disorders related to the stomatognathic system. | NIH “Good” quality. |
| Gawriolek et al. [20] (2014) | This study aimed to analyze the effectiveness of myorelaxation therapy (nocturnal sublingual splint + stretching exercises) in TMD. | Study design: nonrandomized controlled trial N: 78 participants.
| Jaw-tracking examination Computerized mandibular scanner (CMS) Functional examination Active mandibular movements Follow-up: After 4 weeks with no intervention, then 3 weeks, 3 months, and 6 months after treatment | After the treatment, mandibular opening range increased by 8 mm (19%, p < 0.05), lateral movement by 2.1 mm (36%, p < 0.05), while protrusive movement decreased by 0.5 mm (p > 0.05). These results were supported by the decrease in reported impairment and clinical pain occurrence (p < 0.05). | Myorelaxation therapy was effective in the treatment of the patient group. A significant improvement in opening range, lateral movement, and referred pain was achieved after 6 months of treatment. | MINORS 17/24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brighenti, N.; Battaglino, A.; Sinatti, P.; Abuín-Porras, V.; Sánchez Romero, E.A.; Pedersini, P.; Villafañe, J.H. Effects of an Interdisciplinary Approach in the Management of Temporomandibular Disorders: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 2777. https://doi.org/10.3390/ijerph20042777
Brighenti N, Battaglino A, Sinatti P, Abuín-Porras V, Sánchez Romero EA, Pedersini P, Villafañe JH. Effects of an Interdisciplinary Approach in the Management of Temporomandibular Disorders: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(4):2777. https://doi.org/10.3390/ijerph20042777
Chicago/Turabian StyleBrighenti, Nicolò, Andrea Battaglino, Pierluigi Sinatti, Vanesa Abuín-Porras, Eleuterio A. Sánchez Romero, Paolo Pedersini, and Jorge H. Villafañe. 2023. "Effects of an Interdisciplinary Approach in the Management of Temporomandibular Disorders: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 4: 2777. https://doi.org/10.3390/ijerph20042777